Free TB Treatment in the Philippines — DOH DOTS at the RHU (2026)
Libreng TB Treatment sa Pilipinas — DOH DOTS sa RHU (2026)

5 Things to Know
Free TB treatment in five facts.


Quick Summary
Mabilis na Buod
Important Medical Disclaimer: TB is treatable and curable, but treatment requires medical supervision. This guide explains how to ACCESS care — diagnosis and treatment decisions must come from your healthcare provider. Never stop your DOTS regimen on your own; incomplete treatment is the main cause of drug-resistant TB.
Mahalagang Medical Disclaimer: Magagamot ang TB at kayang gumaling, pero kailangan ng medical supervision sa treatment. Itong gabay ay tungkol sa paano i-ACCESS ang treatment — galing sa healthcare provider mo ang diagnosis at treatment decisions. Huwag mong basta hihinto ang DOTS regimen mo; ang hindi tapos na treatment ang pangunahing dahilan ng drug-resistant TB.
Table of Contents
Talaan ng Nilalaman
The Short Answer
Ang Maikling Sagot
Tuberculosis treatment in the Philippines is 100% free under the DOH National Tuberculosis Program (NTP). The standard 6-month DOTS (Directly Observed Treatment, Short-course) regimen — rifampicin (R), isoniazid (H), pyrazinamide (Z), and ethambutol (E) — is provided free at any Rural Health Unit (RHU) or City Health Center. Sputum tests (smear microscopy and GeneXpert MTB/RIF), chest X-ray referral, follow-up monitoring, and even second-line drugs for drug-resistant TB are also free at PMDT-certified facilities. PhilHealth membership is not required for the patient — the drugs come from DOH supply, not your PhilHealth case rate. The catch: TB clinic days vary by RHU (often 2-3 days a week), so call before your first visit.
100% libre ang tuberculosis treatment sa Pilipinas sa ilalim ng DOH National Tuberculosis Program (NTP). Ang standard na 6-buwang DOTS (Directly Observed Treatment, Short-course) regimen — rifampicin (R), isoniazid (H), pyrazinamide (Z), at ethambutol (E) — ay libre sa kahit anong Rural Health Unit (RHU) o City Health Center. Pati ang sputum tests (smear microscopy at GeneXpert MTB/RIF), chest X-ray referral, follow-up monitoring, at second-line drugs para sa drug-resistant TB ay libre rin sa PMDT-certified facilities. Hindi kailangan ng PhilHealth membership para sa pasyente — ang gamot ay galing sa DOH supply, hindi sa PhilHealth case rate mo. Ang catch: nag-iiba ang TB clinic days per RHU (madalas 2-3 araw kada linggo), kaya tumawag muna bago ang first visit.
Symptoms That Should Prompt a Test
Mga Sintomas na Dapat Mag-test
The DOH classifies anyone with these signs as a presumptive TB case who should be screened. Free sputum testing is the entry point — no symptoms threshold, no referral needed.
- Cough lasting 2 weeks or more — the single most important sign. Cough with blood (hemoptysis) is a same-day red flag
- Unexplained weight loss — pants getting loose, no diet change
- Night sweats — drenching enough to change clothes or sheets
- Low-grade fever, especially in the evening — usually under 38.5°C, may come and go for weeks
- Fatigue and loss of appetite — disproportionate to your usual workload
- Chest pain or shortness of breath — when present alongside cough
- Close contact with a confirmed TB case — household member, dorm/jail mate, or co-worker in a small enclosed space, even without symptoms
If you have any of these — especially the 2-week cough — go straight to your RHU. The screening and sputum collection are free; you do not need a doctor's referral to start.
Ang sinumang may ganitong palatandaan ay tinatawag ng DOH na presumptive TB case at dapat i-screen. Ang libreng sputum testing ang entry point — walang symptoms threshold, walang kailangang referral.
- Ubo na 2 linggo o higit pa — ito ang pinakaimportanteng senyales. Ang ubong may dugo (hemoptysis) ay same-day red flag
- Pumapayat nang walang dahilan — lumuluwag ang pantalon, walang diet change
- Pawis sa gabi — nababasa nang husto na kailangan magpalit ng damit o kumot
- Lagnat na hindi mataas, lalo na pag-gabi — karaniwang mababa sa 38.5°C, dumarating at nawawala nang ilang linggo
- Pagod at walang gana kumain — sobra kaysa sa karaniwang ginagawa mo
- Sakit sa dibdib o hirap sa paghinga — kapag kasabay ng ubo
- Malapit na kontak sa confirmed TB case — kasama sa bahay, kuwarto/jail, o katrabaho sa maliit na enclosed space, kahit walang sintomas
Kung mayroon ka ng kahit alin sa mga ito — lalo na ang 2-linggong ubo — pumunta agad sa RHU. Libre ang screening at sputum collection; hindi mo kailangan ng doctor's referral para magsimula.
The Diagnosis Flow at the RHU
Ang Diagnosis Flow sa RHU
From first walk-in to a treatment registration, the standard NTP diagnostic flow looks like this:
1. RHU consult and symptom screening
You'll be triaged at the front desk. Tell them you've been coughing for more than 2 weeks (or describe other symptoms). They will route you to the TB clinic — often a dedicated room or schedule (Tuesdays/Thursdays in many LGUs). The medical officer or nurse will do a brief history and physical exam.
2. Sputum collection (2 samples)
You'll be asked to give two sputum samples:
- Spot sample: Collected on the day of the consult, supervised in a well-ventilated area
- Early morning sample: Collected at home the next morning before brushing teeth (highest bacterial load); brought back to the RHU
You will be given a sterile container with your case number. Cough deeply from the chest — saliva alone is not enough.
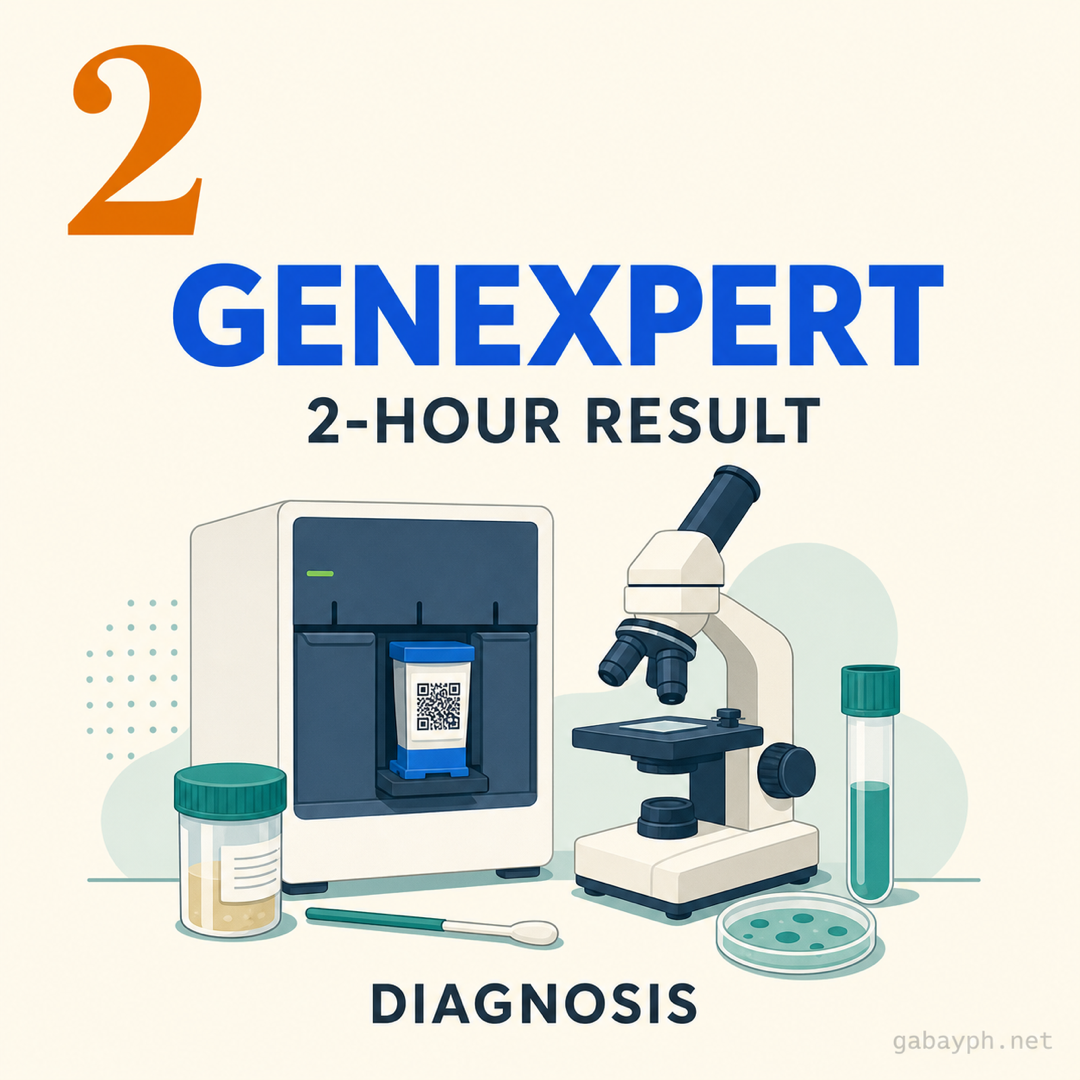
3. Sputum smear microscopy or GeneXpert MTB/RIF
- Sputum smear microscopy: Result in 1-2 days. Available at most RHUs. Confirms acid-fast bacilli (AFB)
- GeneXpert MTB/RIF: Result in about 2 hours. Available at upgraded RHUs and DOH-supported labs. Detects Mycobacterium tuberculosis AND identifies rifampicin resistance in one test — making it the preferred frontline test under current NTP guidance
Both are free. If your RHU doesn't have GeneXpert on-site, they will refer your sample to the nearest DOH-supported lab.
4. Chest X-ray (when needed)
If the sputum result is negative but clinical suspicion remains high, the medical officer may order a chest X-ray. Some RHUs offer this free; others refer to a DOH hospital or partner facility. Bring your case record so the X-ray is processed under the NTP.
5. Diagnosis and treatment registration
Once TB is confirmed, you are registered as a TB patient under the NTP. You will be assigned a treatment supporter (RHU nurse, community health worker, or trained family member), given a TB Treatment Card, and started on the DOTS regimen the same day or within a few days.
Mula sa unang pagpasok hanggang sa treatment registration, ito ang standard na NTP diagnostic flow:
1. RHU consult at symptom screening
Ita-triage ka sa front desk. Sabihin mo na umuubo ka nang mahigit 2 linggo (o ilarawan ang ibang sintomas). Ire-route ka nila sa TB clinic — madalas may dedicated room o schedule (Martes/Huwebes sa maraming LGU). Magsasagawa ng brief history at physical exam ang medical officer o nurse.
2. Sputum collection (2 sample)
Hihingin sa iyo ng dalawang sputum sample:
- Spot sample: Kinukuha sa araw ng consult, supervised sa well-ventilated na lugar
- Early morning sample: Kinukuha sa bahay nang sumunod na umaga bago magsipilyo (pinakamataas ang bacterial load); dinadala pabalik sa RHU
Bibigyan ka ng sterile container na may case number mo. Umubo nang malalim mula sa dibdib — hindi sapat ang laway lang.
3. Sputum smear microscopy o GeneXpert MTB/RIF
- Sputum smear microscopy: Resulta sa 1-2 araw. Available sa karamihan ng RHU. Kinukumpirma ang acid-fast bacilli (AFB)
- GeneXpert MTB/RIF: Resulta sa mga 2 oras. Available sa upgraded RHU at DOH-supported labs. Nade-detect ang Mycobacterium tuberculosis AT na-identify ang rifampicin resistance sa isang test — kaya ito ang preferred frontline test sa current NTP guidance
Libre pareho. Kung walang GeneXpert sa RHU mo, ire-refer nila ang sample mo sa pinakamalapit na DOH-supported lab.
4. Chest X-ray (kung kailangan)
Kung negative ang sputum result pero matindi pa rin ang clinical suspicion, pwedeng mag-order ng chest X-ray ang medical officer. May RHU na libre ito; may iba na nagre-refer sa DOH hospital o partner facility. Dalhin ang case record mo para ma-process ang X-ray sa ilalim ng NTP.
5. Diagnosis at treatment registration
Pag na-kumpirma ang TB, maire-register ka bilang TB patient sa ilalim ng NTP. Bibigyan ka ng treatment supporter (RHU nurse, community health worker, o trained family member), ibibigay ang TB Treatment Card, at magsisimula sa DOTS regimen sa parehong araw o sa loob ng ilang araw.
The 6-Month DOTS Regimen
Ang 6-Buwang DOTS Regimen
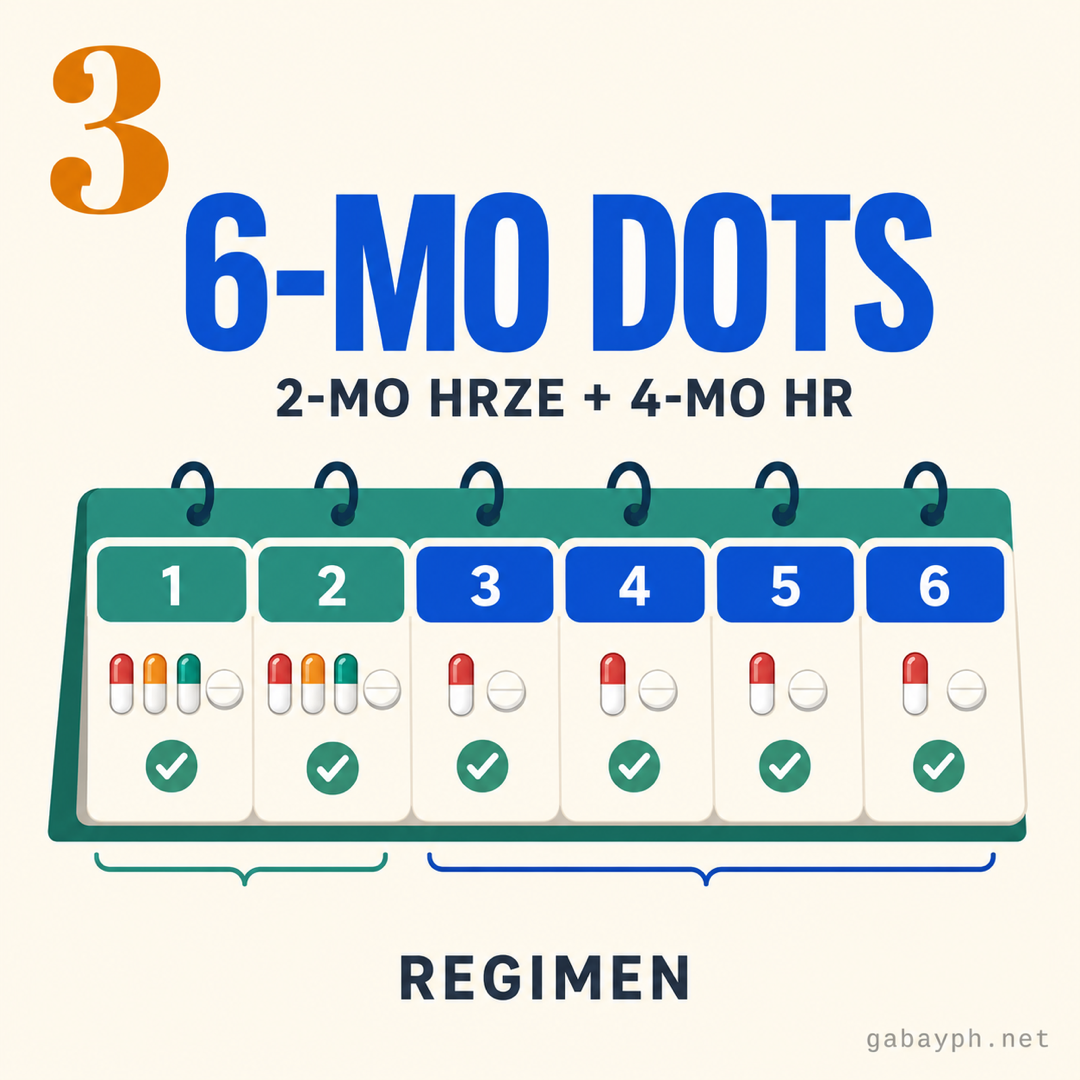
For drug-susceptible TB (the most common case), the WHO-standard regimen — adopted by the DOH NTP — runs for 6 months in two phases. All drugs are provided free by the RHU.
Intensive phase (2 months) — HRZE daily
- H — Isoniazid
- R — Rifampicin
- Z — Pyrazinamide
- E — Ethambutol
Taken daily, usually as a fixed-dose combination (FDC) tablet to simplify pill burden. Dose is weight-based. During this phase, the bacterial load drops sharply — the 2-week threshold is widely cited as the point at which most drug-susceptible TB patients with good clinical response are generally treated as non-infectious, though this varies by individual and only your physician can clear you.
Continuation phase (4 months) — HR daily
- H — Isoniazid
- R — Rifampicin
You continue daily for 4 more months to wipe out the remaining slow-growing bacilli. This phase is where most people feel "fine" and are tempted to stop — don't. Stopping early is the #1 cause of TB relapse and the main pathway to drug-resistant TB.
What DOT (Directly Observed Treatment) means in practice
You take your medications in front of a treatment supporter — usually an RHU nurse, a barangay health worker, or a trained family member designated by the RHU. The treatment supporter signs your TB Treatment Card every time you take a dose. Two common arrangements:
- Facility-based DOT: You go to the RHU daily (some areas allow every-other-day or weekday-only depending on policy)
- Community-based DOT: A community health worker visits you at home, or a trained family member acts as supporter under RHU monitoring — common in remote areas or for patients with mobility issues
Follow-up sputum tests are scheduled at the end of month 2 (to check conversion from positive to negative) and at the end of treatment (to confirm cure). Both are free.
Para sa drug-susceptible TB (ang pinakakaraniwang kaso), ang WHO-standard regimen — sinunod ng DOH NTP — ay tumatakbo nang 6 buwan sa dalawang phase. Libre lahat ng gamot mula sa RHU.
Intensive phase (2 buwan) — HRZE araw-araw
- H — Isoniazid
- R — Rifampicin
- Z — Pyrazinamide
- E — Ethambutol
Iniinom araw-araw, karaniwang fixed-dose combination (FDC) tablet para mas konti ang pill burden. Weight-based ang dose. Sa phase na ito, bumababa nang husto ang bacterial load — ang 2-linggong threshold ang madalas i-cite bilang puntong itinuturing nang generally non-infectious ang karamihan ng drug-susceptible TB patients na may good clinical response, bagama't iba-iba ito kada indibidwal at ang doktor mo lang ang makakapag-clear sa iyo.
Continuation phase (4 buwan) — HR araw-araw
- H — Isoniazid
- R — Rifampicin
Ituloy ang araw-araw na pag-inom nang 4 pang buwan para matanggal ang natitirang slow-growing bacilli. Sa phase na ito nakakaramdam na ng "ayos na" ang karamihan at gustong tumigil — huwag. Ang maagang paghinto ang #1 na dahilan ng TB relapse at ang pangunahing daan papunta sa drug-resistant TB.
Ano ang DOT (Directly Observed Treatment) sa practice
Iniinom mo ang gamot sa harap ng treatment supporter — karaniwang RHU nurse, barangay health worker, o trained family member na itinalaga ng RHU. Pumipirma ang treatment supporter sa TB Treatment Card mo tuwing iniinom mo ang dose. Dalawang common arrangement:
- Facility-based DOT: Pumupunta ka sa RHU araw-araw (may lugar na pinapayagan ang every-other-day o weekday-only depende sa policy)
- Community-based DOT: Bumibisita sa iyo sa bahay ang community health worker, o trained family member na nag-a-act bilang supporter sa ilalim ng RHU monitoring — common sa malayong lugar o para sa pasyenteng may mobility issues
Iniiskedyul ang follow-up sputum tests sa katapusan ng buwan 2 (para tingnan ang conversion mula positive papuntang negative) at sa katapusan ng treatment (para kumpirmahin ang cure). Libre pareho.
What's Free Under the NTP
Anong Libre sa NTP
Everything in the standard TB care pathway is covered. You should not be charged any of the following at an RHU, city health center, or DOH-supported NTP facility:
- Initial consult and symptom screening
- Sputum smear microscopy (acid-fast bacilli / AFB)
- GeneXpert MTB/RIF molecular test — includes rifampicin resistance detection
- Chest X-ray — free at many RHUs; referral to a DOH-supported facility otherwise (still free under the NTP referral)
- First-line drugs: rifampicin (R), isoniazid (H), pyrazinamide (Z), ethambutol (E) — full 6-month supply
- Vitamin B6 (pyridoxine) supplementation — given alongside isoniazid to prevent peripheral neuropathy
- Treatment supporter supervision and DOT visits
- Follow-up sputum tests at month 2 and end of treatment
- Liver function test (LFT) monitoring when clinically indicated
- TB Treatment Card and case registration under the NTP
Where does PhilHealth fit in?
PhilHealth has a TB-DOTS Package with case rates historically set around ₱4,000 (intensive phase) and ₱2,500 (continuation phase) per PhilHealth Circular 2019-0013 — verify the current amounts at philhealth.gov.ph, as PhilHealth revises benefit packages periodically. This case rate is paid to the facility (RHU or DOTS center), not to the patient directly. It helps fund the facility's operations — your drugs and tests still come from DOH supply free of charge regardless. You do not need PhilHealth membership to receive treatment. If you happen to be a member, the facility may file the claim on your behalf, but it does not change what you receive.
Sakop ang lahat sa standard TB care pathway. Hindi ka dapat sininingil ng kahit alin sa mga sumusunod sa RHU, city health center, o DOH-supported NTP facility:
- Initial consult at symptom screening
- Sputum smear microscopy (acid-fast bacilli / AFB)
- GeneXpert MTB/RIF molecular test — kasama ang rifampicin resistance detection
- Chest X-ray — libre sa maraming RHU; referral sa DOH-supported facility kung wala (libre pa rin sa ilalim ng NTP referral)
- First-line drugs: rifampicin (R), isoniazid (H), pyrazinamide (Z), ethambutol (E) — buong 6-buwang supply
- Vitamin B6 (pyridoxine) supplementation — kasabay ng isoniazid para iwasan ang peripheral neuropathy
- Treatment supporter supervision at DOT visits
- Follow-up sputum tests sa month 2 at end of treatment
- Liver function test (LFT) monitoring kapag clinically indicated
- TB Treatment Card at case registration sa NTP
Saan papasok ang PhilHealth?
May TB-DOTS Package ang PhilHealth na may case rates na historically nakatakda sa paligid ng ₱4,000 (intensive phase) at ₱2,500 (continuation phase) per PhilHealth Circular 2019-0013 — i-verify ang current amounts sa philhealth.gov.ph dahil paminsan-minsan ay nagre-revise ang PhilHealth ng benefit packages. Ang case rate ay binabayaran sa facility (RHU o DOTS center), hindi direkta sa pasyente. Tumutulong ito sa operations ng facility — galing pa rin sa DOH supply ang gamot at tests mo nang libre. Hindi mo kailangan ng PhilHealth membership para makatanggap ng treatment. Kung member ka naman, pwedeng i-file ng facility ang claim para sa iyo, pero hindi nito babaguhin ang matatanggap mo.
MDR-TB Pathway (PMDT)
MDR-TB Pathway (PMDT)
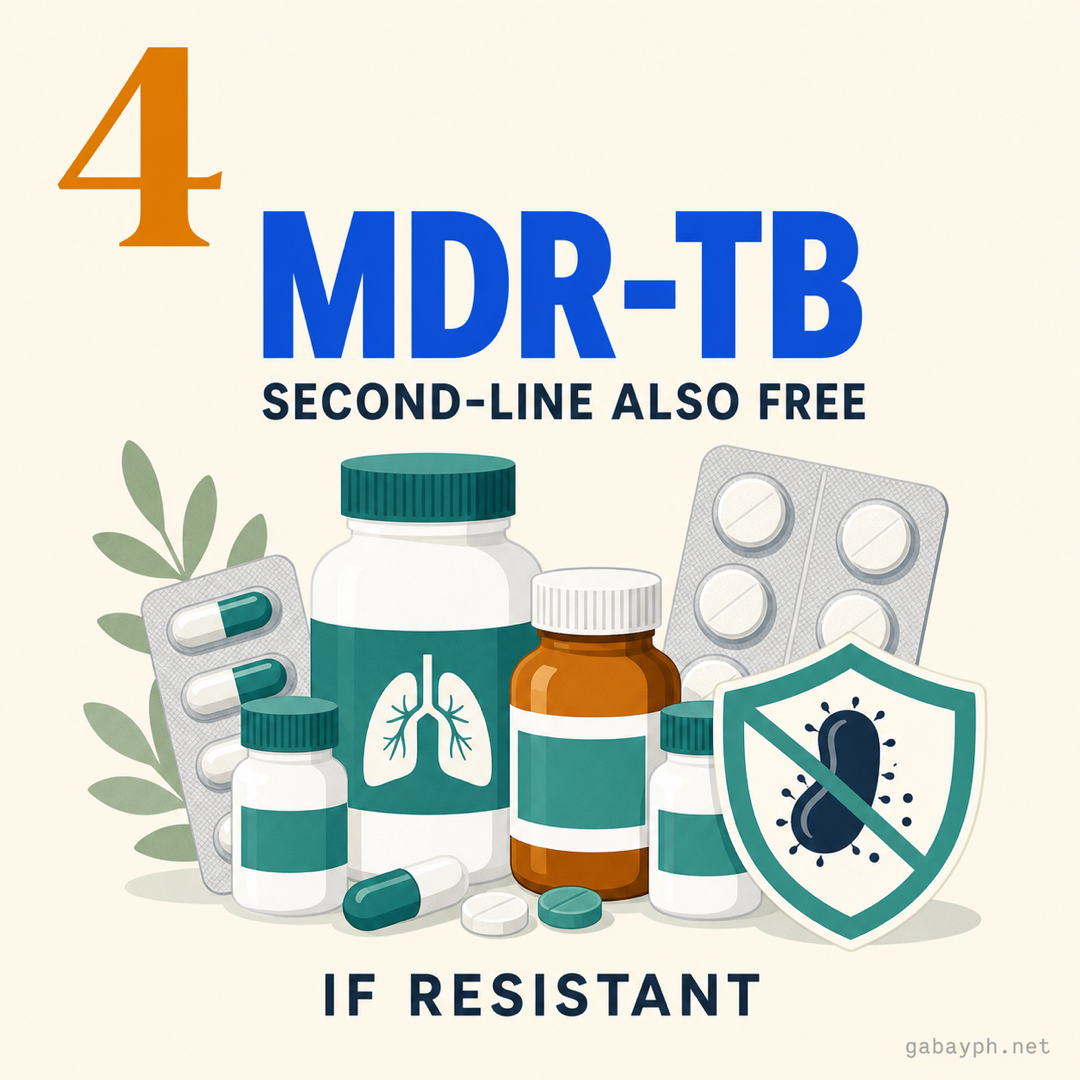
Multidrug-resistant TB (MDR-TB) is TB that doesn't respond to at least isoniazid and rifampicin — the two strongest first-line drugs. The DOH manages this through the Programmatic Management of Drug-Resistant TB (PMDT), and treatment is also fully free.
How MDR-TB gets caught
GeneXpert MTB/RIF flags rifampicin resistance in the same 2-hour test that confirms TB. Resistance to other first-line drugs is detected through additional drug susceptibility testing (DST) at DOH reference labs. If you're flagged as MDR-TB, the RHU refers you to a PMDT-certified facility — there are PMDT treatment centers in every region, often based at provincial or DOH-retained hospitals.
The MDR-TB regimen
Modern shorter regimens for MDR-TB run 9 to 12 months, replacing the older 18-24 month regimens. They use combinations of newer drugs, including bedaquiline and (for extensively drug-resistant TB / XDR-TB) delamanid. All of these are provided free under the PMDT — they would otherwise cost hundreds of thousands of pesos out of pocket.
What's free under the PMDT
- GeneXpert MTB/RIF and full drug susceptibility testing
- Second-line and newer drugs (bedaquiline, delamanid, linezolid, levofloxacin, moxifloxacin, clofazimine, others as prescribed)
- Monitoring labs: monthly LFTs, ECG (for cardiac side effects from some regimens), audiometry (for older injectable-containing regimens)
- Treatment supporter and case management
- Patient enabler support packages (food allowance, transport reimbursement) in many PMDT centers — ask
If you cannot afford the transport to a PMDT center, the RHU can usually coordinate referral with the local social welfare office (DSWD) or barangay for assistance. Don't delay starting treatment — MDR-TB is harder to cure the longer it goes untreated.
Ang multidrug-resistant TB (MDR-TB) ay TB na hindi tumutugon sa kahit isoniazid at rifampicin — ang dalawang pinakamalakas na first-line drugs. Pinamamahalaan ito ng DOH sa pamamagitan ng Programmatic Management of Drug-Resistant TB (PMDT), at libre rin nang buo ang treatment.
Paano nahuhuli ang MDR-TB
Nakikita ng GeneXpert MTB/RIF ang rifampicin resistance sa parehong 2-oras na test na kumukumpirma ng TB. Ang resistance sa ibang first-line drugs ay nadidetect sa karagdagang drug susceptibility testing (DST) sa DOH reference labs. Kapag na-flag ka bilang MDR-TB, ire-refer ka ng RHU sa PMDT-certified facility — may PMDT treatment centers sa bawat region, madalas naka-base sa provincial o DOH-retained hospitals.
Ang MDR-TB regimen
Ang modern shorter regimens para sa MDR-TB ay tumatakbo ng 9 hanggang 12 buwan, kapalit ng mas lumang 18-24 buwang regimens. Gumagamit sila ng kumbinasyon ng mas bagong gamot, kasama ang bedaquiline at (para sa extensively drug-resistant TB / XDR-TB) delamanid. Libre lahat ito sa ilalim ng PMDT — magkakahalaga ito ng daan-daang libong piso kung sariling bulsa.
Anong libre sa PMDT
- GeneXpert MTB/RIF at full drug susceptibility testing
- Second-line at mas bagong gamot (bedaquiline, delamanid, linezolid, levofloxacin, moxifloxacin, clofazimine, iba pa kung naka-prescribe)
- Monitoring labs: monthly LFTs, ECG (para sa cardiac side effects ng ibang regimens), audiometry (para sa mas lumang injectable-containing regimens)
- Treatment supporter at case management
- Patient enabler support packages (food allowance, transport reimbursement) sa maraming PMDT center — itanong
Kung hindi mo kayang bayaran ang transport papunta sa PMDT center, kayang i-coordinate ng RHU ang referral sa local social welfare office (DSWD) o barangay para sa tulong. Huwag i-delay ang pagsisimula ng treatment — mas mahirap pagalingin ang MDR-TB kapag matagal nang hindi nagagamot.
Side Effects to Watch
Side Effects na Bantayan
Most people tolerate the standard DOTS regimen well, but a few side effects are common enough to mention so you know what's normal and what needs a same-day call to your treatment supporter.
- Orange/reddish urine, sweat, or tears (rifampicin): Normal and harmless. The dye is the drug being excreted. Avoid wearing your favorite white shirt to bed for the first few weeks; soft contact lenses may stain
- Tingling or numbness in hands/feet (isoniazid, peripheral neuropathy): Largely prevented by Vitamin B6 (pyridoxine), which the RHU dispenses alongside your DOTS drugs. If it appears, tell the medical officer — the B6 dose can be adjusted
- Joint pain, especially in toes/big toe (pyrazinamide, hyperuricemia): Drink plenty of water and reduce purine-heavy food (organ meats, anchovies). Severe joint pain warrants a same-day call
- Visual changes — blurry vision or trouble distinguishing red/green (ethambutol): Rare but serious. Stop the dose and call your doctor or RHU the same day. Visual changes are usually reversible if caught early
- Nausea, loss of appetite, abdominal pain (any drug, but watch the liver): Mild nausea is common in the first 2 weeks. Yellowing of the eyes or skin, dark "tea-colored" urine combined with pale stools, or persistent vomiting can signal drug-induced hepatitis — stop and seek same-day care
- Skin rash or itching: Mild rash can be managed; widespread rash with fever or peeling needs immediate medical attention
Monthly liver function tests (LFTs) are recommended during the intensive phase, especially if you have pre-existing liver disease, are over 60, are heavily underweight, or drink alcohol. These are typically covered under the NTP referral.
Avoid alcohol throughout treatment — it amplifies liver toxicity from all four first-line drugs.
Karamihan ng tao ay kayang tiisin ang standard DOTS regimen, pero may ilang side effects na common kaya nababanggit para alam mo kung ano ang normal at ano ang kailangan ng same-day call sa treatment supporter mo.
- Orange/mapulang ihi, pawis, o luha (rifampicin): Normal at hindi nakakasama. Ang kulay ay galing sa gamot na lumalabas. Iwasan ang puting damit pag-tulog sa unang ilang linggo; pwedeng magkamantsa ang soft contact lenses
- Pangangalay o pamamanhid ng kamay/paa (isoniazid, peripheral neuropathy): Karaniwang iniiwasan ng Vitamin B6 (pyridoxine), na ipinapamahagi ng RHU kasabay ng DOTS drugs mo. Kung lumitaw, sabihin sa medical officer — pwedeng i-adjust ang B6 dose
- Sakit ng kasukasuan, lalo na sa daliri ng paa/hinlalaki (pyrazinamide, hyperuricemia): Uminom ng maraming tubig at bawasan ang purine-heavy na pagkain (laman-loob, dilis). Ang matinding joint pain ay nangangailangan ng same-day call
- Pagbabago sa paningin — malabo o hirap mag-distinguish ng pula/berde (ethambutol): Bihira pero seryoso. Itigil ang dose at tumawag sa doktor o RHU sa parehong araw. Karaniwang reversible ang visual changes kapag nahuli nang maaga
- Pagkahilo, walang gana kumain, sakit ng tiyan (kahit anong gamot, pero bantayan ang atay): Common sa unang 2 linggo ang banayad na pagkahilo. Ang paninilaw ng mata o balat, maitim na "tea-colored" na ihi kasama ng mapuputlang dumi, o paulit-ulit na pagsusuka ay pwedeng maging senyales ng drug-induced hepatitis — itigil at humingi ng same-day care
- Pantal o pangangati ng balat: Kayang i-manage ang banayad na pantal; ang malawak na pantal na may lagnat o nababalat na balat ay nangangailangan ng agarang medical attention
Inirerekomenda ang monthly liver function tests (LFTs) sa intensive phase, lalo na kung may dati nang sakit sa atay, mahigit 60 ka, sobrang payat, o umiinom ng alkohol. Karaniwang sakop ito sa NTP referral.
Iwasan ang alkohol sa buong treatment — nadadagdagan nito ang liver toxicity mula sa apat na first-line drugs.
Work, Family, and Close Contacts
Trabaho, Pamilya, at Close Contacts
Can I keep working?
For most cases of drug-susceptible pulmonary TB, the 2-week threshold of consistent DOTS treatment is widely cited as the point at which an individual with good clinical response (cough improving, no fever) is generally treated as non-infectious. This is a general guideline, not a guarantee — only your physician can clear you for return-to-work, and that clearance depends on your specific bacterial load, smear status, drug susceptibility, and clinical response. Office and remote work usually resume sooner than physical labor or jobs in tightly enclosed spaces. Most employers ask for a fit-to-work certificate; your RHU medical officer must be the one to issue it.
Under the Labor Code's sickness benefit provisions and SSS sickness benefit (if you're a member), you may also be entitled to paid sick leave or daily sickness allowance during the period of incapacity — see our SSS guide for the claim process.
What about my family and household?
The DOH NTP strongly recommends household contact screening. Anyone who has lived with you in the same dwelling — especially children under 5 and people with diabetes, HIV, or other immunocompromising conditions — should be screened at the RHU. This is also free.
- Adults with symptoms: Sputum testing under the same NTP flow
- Asymptomatic adult contacts: May still be evaluated for latent TB infection; in selected cases, TB preventive treatment (TPT) is offered
- Children under 5 in contact with a confirmed TB case: Often started on TB preventive treatment (isoniazid for several months) even without active disease, per current DOH/WHO guidance
What if I miss doses?
Missing occasional doses can be made up under treatment supporter guidance — but missing more than a few in a row threatens cure and breeds drug resistance. If you miss a dose, tell your treatment supporter the same day. If you miss more than a week, the RHU may need to extend or restart your regimen depending on which phase you're in. The TB Treatment Card exists specifically to catch and correct this.
Pwede ba akong magtrabaho?
Para sa karamihan ng kaso ng drug-susceptible pulmonary TB, ang 2-linggong threshold ng consistent DOTS treatment ay madalas i-cite bilang puntong itinuturing nang generally non-infectious ang taong may good clinical response (umaayos ang ubo, walang lagnat). General guideline lang ito, hindi garantiya — ang doktor mo lang ang makakapag-clear sa iyo para mag-return-to-work, at depende ang clearance sa specific bacterial load, smear status, drug susceptibility, at clinical response mo. Ang office at remote work ay karaniwang mas mabilis na nagre-resume kaysa sa physical labor o trabaho sa masikip na enclosed space. Karamihan ng employer ay humihingi ng fit-to-work certificate; ang RHU medical officer mo lang dapat ang mag-issue nito.
Sa ilalim ng sickness benefit provisions ng Labor Code at SSS sickness benefit (kung member ka), pwede ka ring maging entitled sa paid sick leave o daily sickness allowance sa period ng incapacity — tingnan ang aming SSS guide para sa claim process.
Paano ang pamilya at sambahayan ko?
Malakas na inirerekomenda ng DOH NTP ang household contact screening. Ang sinumang nakatira mo sa parehong bahay — lalo na ang mga batang under 5 at taong may diabetes, HIV, o ibang immunocompromising condition — ay dapat i-screen sa RHU. Libre rin ito.
- Adults na may sintomas: Sputum testing sa parehong NTP flow
- Asymptomatic adult contacts: Pwede pa ring i-evaluate para sa latent TB infection; sa selected cases, ino-offer ang TB preventive treatment (TPT)
- Mga batang under 5 na may contact sa confirmed TB case: Madalas pinapasimulan sa TB preventive treatment (isoniazid sa ilang buwan) kahit walang active disease, ayon sa current DOH/WHO guidance
Paano kung may na-miss akong dose?
Pwedeng habulin ang occasional missed dose sa ilalim ng treatment supporter guidance — pero ang mawalan ng higit sa ilang doses na magkakasunod ay nagre-risk ng cure at nagpapalakas ng drug resistance. Kung nakaligtaan mo ang dose, sabihin sa treatment supporter sa parehong araw. Kung lumampas ng isang linggo, pwedeng kailangang i-extend o i-restart ng RHU ang regimen mo depende sa phase. Ang TB Treatment Card ay umiiral specifically para mahuli at maitama ito.
Pro Tips
Mga Payo
- Call your RHU before your first visit. TB clinic days are not daily in most RHUs — many run on Tuesdays/Thursdays only. A 30-second call saves you a wasted trip and confirms whether GeneXpert is on-site or your sputum will be referred out.
- Designate a treatment supporter early. Successful cure depends on consistent DOT. If you cannot go to the RHU daily (work hours, mobility, distance), discuss community-based DOT or a trained family supporter at registration — not midway through treatment. The earlier this is set, the cleaner your TB Treatment Card stays.
- Bring the same morning sputum container back unwashed. Sounds obvious; people forget. The container is sterile, labeled with your case number, and meant to be returned with the morning sample inside — not rinsed or refilled into a different bottle.
- Take your meds at the same time every day. Most patients do well taking the FDC tablet in the morning on an empty stomach (rifampicin absorbs better) with a glass of water. Set a phone alarm — daily consistency is the entire point of "directly observed."
- Keep your TB Treatment Card on you. If you travel, transfer LGUs, or end up at another facility, the card is your proof of regimen and progress. The receiving RHU/PMDT can pick up your treatment without restarting if the card is current.
- Do not buy TB drugs at private pharmacies "to skip the RHU schedule." Self-administered TB treatment without DOT supervision is the textbook recipe for drug-resistant TB. The drugs are free at the RHU specifically so cost isn't your reason to skip supervision.
- Tumawag sa RHU mo bago ang first visit. Hindi araw-araw ang TB clinic days sa karamihan ng RHU — maraming Martes/Huwebes lamang. 30-second call ay nakakaiwas sa wasted trip at kumukumpirma kung on-site ang GeneXpert o ire-refer out ang sputum mo.
- Mag-designate ng treatment supporter agad. Nakadepende sa consistent DOT ang successful cure. Kung hindi ka makapunta sa RHU araw-araw (work hours, mobility, distansya), pag-usapan ang community-based DOT o trained family supporter sa registration — hindi sa kalagitnaan ng treatment. Kapag maaga itong na-set, mas malinis ang TB Treatment Card mo.
- Ibalik ang parehong morning sputum container nang hindi hinuhugasan. Mukhang obvious; nakakalimutan ng tao. Sterile ang container, naka-label na may case number mo, at meant na ibalik na may morning sample sa loob — hindi binabanlawan o nilipat sa ibang bote.
- Inumin ang gamot sa parehong oras araw-araw. Karamihan ng pasyente ay maayos pag-inom ng FDC tablet sa umaga, walang laman ang sikmura (mas mahusay na sinasalo ng katawan ang rifampicin), na may isang basong tubig. Mag-set ng phone alarm — daily consistency ang buong punto ng "directly observed."
- Dalhin lagi ang TB Treatment Card. Kung magbiyahe ka, lumipat ng LGU, o mapunta sa ibang facility, ang card ang proof ng regimen at progress mo. Kayang ituloy ng receiving RHU/PMDT ang treatment nang walang restart kung up-to-date ang card.
- Huwag bumili ng TB drugs sa private pharmacy "para iwasan ang RHU schedule." Ang self-administered TB treatment na walang DOT supervision ay textbook recipe para sa drug-resistant TB. Libre ang gamot sa RHU specifically para hindi gastos ang dahilan mo para iwasan ang supervision.
Frequently Asked Questions
Mga Madalas Itanong
Do I really not have to pay anything?
For TB drugs, sputum tests, GeneXpert, and the standard NTP services at an RHU or DOH-supported facility — yes, nothing. Where small out-of-pocket costs may appear: transport to the facility, optional private chest X-rays if your RHU refers out to a non-DOH partner, or unrelated medications. If you are ever asked to pay for first-line TB drugs at a public facility, that is a red flag — escalate to the City/Provincial Health Officer or DOH Regional Office.
Talagang walang babayaran?
Para sa TB drugs, sputum tests, GeneXpert, at standard NTP services sa RHU o DOH-supported facility — oo, wala. Kung saan pwedeng lumitaw ang maliit na out-of-pocket: transport papunta sa facility, optional na private chest X-rays kung nagre-refer ang RHU mo sa non-DOH partner, o gamot na walang kinalaman sa TB. Kung sinisingil ka para sa first-line TB drugs sa public facility, red flag iyan — i-escalate sa City/Provincial Health Officer o DOH Regional Office.
Can I go to an RHU outside my barangay or LGU?
Yes. The NTP is national, and RHUs do not strictly residency-gate TB services. Many people choose an RHU near their workplace instead of their home for daily DOT convenience. If you do switch facilities, ask the original RHU for a transfer form and bring your TB Treatment Card so your case continues seamlessly without restarting the regimen.
Pwede ba akong pumunta sa RHU na hindi sa barangay o LGU ko?
Oo. National ang NTP, at hindi strict ang residency-gating ng mga RHU sa TB services. Maraming tao ang pumipili ng RHU malapit sa trabaho imbes na sa bahay para sa convenience ng daily DOT. Kung magpapalit ka ng facility, hingin ang transfer form sa unang RHU at dalhin ang TB Treatment Card mo para tuloy-tuloy ang kaso mo nang walang restart sa regimen.
What if I don't have PhilHealth?
You can still receive full TB treatment for free. The TB-DOTS Package case rate (₱4,000 + ₱2,500) is paid by PhilHealth to the facility, not to the patient — so PhilHealth membership funds the facility's operations but does not change what you receive. Your DOTS drugs and tests come from DOH supply regardless. If you'd like to enrol in PhilHealth anyway, see our PhilHealth guide.
Paano kung wala akong PhilHealth?
Pwede ka pa ring makatanggap ng buong libreng TB treatment. Ang TB-DOTS Package case rate (₱4,000 + ₱2,500) ay binabayaran ng PhilHealth sa facility, hindi sa pasyente — kaya pinopondohan ng PhilHealth membership ang operations ng facility pero hindi nito babaguhin ang matatanggap mo. Galing pa rin sa DOH supply ang DOTS drugs at tests mo. Kung gusto mong magpa-enrol sa PhilHealth, tingnan ang aming PhilHealth guide.
What's the difference between sputum smear and GeneXpert?
Both are sputum-based tests, but they're different technologies. Sputum smear microscopy looks for acid-fast bacilli (AFB) under a microscope — result in 1-2 days, sensitive enough to detect moderate-to-high bacterial loads. GeneXpert MTB/RIF is a molecular test (PCR-based) that detects M. tuberculosis DNA and simultaneously tests for rifampicin resistance in about 2 hours. GeneXpert is more sensitive and the preferred frontline test under current NTP guidance; smear is still used widely where GeneXpert isn't on-site. Both are free.
Anong pagkakaiba ng sputum smear at GeneXpert?
Pareho silang sputum-based tests, pero magkaibang teknolohiya. Ang sputum smear microscopy ay naghahanap ng acid-fast bacilli (AFB) sa ilalim ng mikroskopyo — resulta sa 1-2 araw, sapat ang sensitivity para sa moderate-to-high na bacterial load. Ang GeneXpert MTB/RIF ay molecular test (PCR-based) na nade-detect ang DNA ng M. tuberculosis at sabay nasa-test ang rifampicin resistance sa mga 2 oras. Mas sensitive ang GeneXpert at ito ang preferred frontline test sa current NTP guidance; ginagamit pa rin ang smear sa maraming lugar kung saan walang on-site na GeneXpert. Libre pareho.
I'm pregnant. Can I still take TB drugs?
Yes — first-line TB drugs (rifampicin, isoniazid, ethambutol, and pyrazinamide) are considered safe in pregnancy by the WHO and DOH, and untreated TB is more dangerous to both mother and baby than the treatment. Vitamin B6 supplementation alongside isoniazid is especially important in pregnancy. Streptomycin (an older injectable) is avoided. Tell the RHU you're pregnant at registration so your regimen and monitoring are tailored. Coordinate with your OB-GYN and the RHU together.
Buntis ako. Pwede ba akong uminom ng TB drugs?
Oo — ang first-line TB drugs (rifampicin, isoniazid, ethambutol, at pyrazinamide) ay itinuturing na ligtas sa pagbubuntis ng WHO at DOH, at mas mapanganib sa nanay at sanggol ang hindi nagagamot na TB kaysa sa treatment. Lalong importante ang Vitamin B6 supplementation kasabay ng isoniazid sa pagbubuntis. Iniiwasan ang streptomycin (mas lumang injectable). Sabihin sa RHU na buntis ka sa registration para ma-tailor ang regimen at monitoring mo. Mag-coordinate sa OB-GYN at RHU nang sabay.
Will my employer find out I have TB?
Your medical information is protected under the Data Privacy Act (RA 10173) and standard medical confidentiality. The RHU cannot disclose your TB status to your employer without your consent. If you need a fit-to-work or back-to-work certificate, the medical officer can issue one without specifying the diagnosis if you ask. Workplace disclosure is your choice — though for jobs in healthcare, food service, or tightly enclosed group settings, voluntary early disclosure plus the 2-week non-infectious threshold usually works in your favor.
Malalaman ba ng employer ko na may TB ako?
Protektado ang medical information mo sa ilalim ng Data Privacy Act (RA 10173) at standard medical confidentiality. Hindi pwedeng ihayag ng RHU ang TB status mo sa employer mo nang walang consent. Kung kailangan mo ng fit-to-work o back-to-work certificate, pwedeng mag-issue ang medical officer nang hindi tinatakda ang diagnosis kung hihingin mo. Choice mo ang workplace disclosure — bagama't para sa trabaho sa healthcare, food service, o masikip na group settings, ang voluntary na maagang pagsasabi kasabay ng 2-linggong non-infectious threshold ay karaniwang nakatutulong sa iyo.
What if I have HIV or diabetes alongside TB?
TB-HIV and TB-diabetes are common dual diagnoses, and the DOH NTP coordinates with the National HIV/AIDS Program and diabetes care pathways. Treatment is still free, but your regimen and follow-up will be more closely monitored. For TB-HIV co-infection, antiretroviral therapy (ART) is started or continued alongside DOTS — disclosure to the RHU TB officer is essential because some HIV drugs interact with rifampicin. For diabetics, tighter glucose control improves TB cure rates and shortens recovery. Tell the RHU your full medical history at registration.
Paano kung may HIV o diabetes ako kasabay ng TB?
Common ang TB-HIV at TB-diabetes na dual diagnosis, at nag-coo-coordinate ang DOH NTP sa National HIV/AIDS Program at diabetes care pathways. Libre pa rin ang treatment, pero mas malapit na mamo-monitor ang regimen at follow-up mo. Para sa TB-HIV co-infection, sinisimulan o ipinagpapatuloy ang antiretroviral therapy (ART) kasabay ng DOTS — mahalaga ang disclosure sa RHU TB officer dahil may HIV drugs na may interaction sa rifampicin. Para sa may diabetes, mas mahigpit na glucose control ay nagpapabuti ng TB cure rates at nagpapaikli ng recovery. Sabihin sa RHU ang full medical history mo sa registration.
What if I'm worried about supply shortages?
DOH first-line TB drug supply is generally stable, but stock-outs at individual RHUs do happen occasionally. If your RHU is temporarily out of a specific drug, options are: (1) ask the RHU to source from a neighbouring LGU's stock under regional DOH coordination, (2) request transfer to a nearby DOTS facility that has stock, or (3) verify with the DOH Regional Office. Never stop or skip doses while waiting — even short interruptions favor drug-resistant TB.
Paano kung nag-aalala ako sa supply shortages?
Karaniwang stable ang DOH first-line TB drug supply, pero may stock-outs sa individual RHUs na nangyayari paminsan-minsan. Kung pansamantalang ubos ang specific drug sa RHU mo, ang options ay: (1) hilingin sa RHU na kumuha ng stock galing sa kalapit na LGU sa ilalim ng regional DOH coordination, (2) hilingin ang transfer sa kalapit na DOTS facility na may stock, o (3) i-verify sa DOH Regional Office. Huwag tumigil o lumaktaw ng dose habang naghihintay — kahit maikling pag-iinterrupt ay paborable sa drug-resistant TB.